
Nearly 1 in every 7 health insurance claims filed in India has some element of fraud in it. That is not a guess. It is an industry estimate that insurers and TPAs are now working with. And from April 1, 2026, the rules for catching that fraud got a lot stricter.
A TPA investigator in Mumbai once caught two hospitalisation claims filed in the same week — identical procedure codes, overlapping admission dates, different policy numbers, but the same attendant phone number on both. Manual review caught it, but only after ₹4.2 lakh had already been pre-authorised. That kind of near-miss is exactly what India's insurers are now under pressure to prevent, not recover from.
Cases like these show why manual reviews alone are no longer enough. As fraud becomes more sophisticated and claim volumes continue to rise, insurers, TPAs, and hospitals need faster and more reliable ways to identify suspicious claims without delaying genuine ones.
Fraud analytics software helps insurers, TPAs, and hospitals detect suspicious health insurance claims before payouts using automated rules, data analysis, and AI-driven risk scoring. As claim volumes increase and fraud becomes more sophisticated, these platforms have become essential for reducing financial losses, improving claims efficiency, and meeting IRDAI's latest fraud monitoring requirements.
What Is Health Insurance Fraud in India?
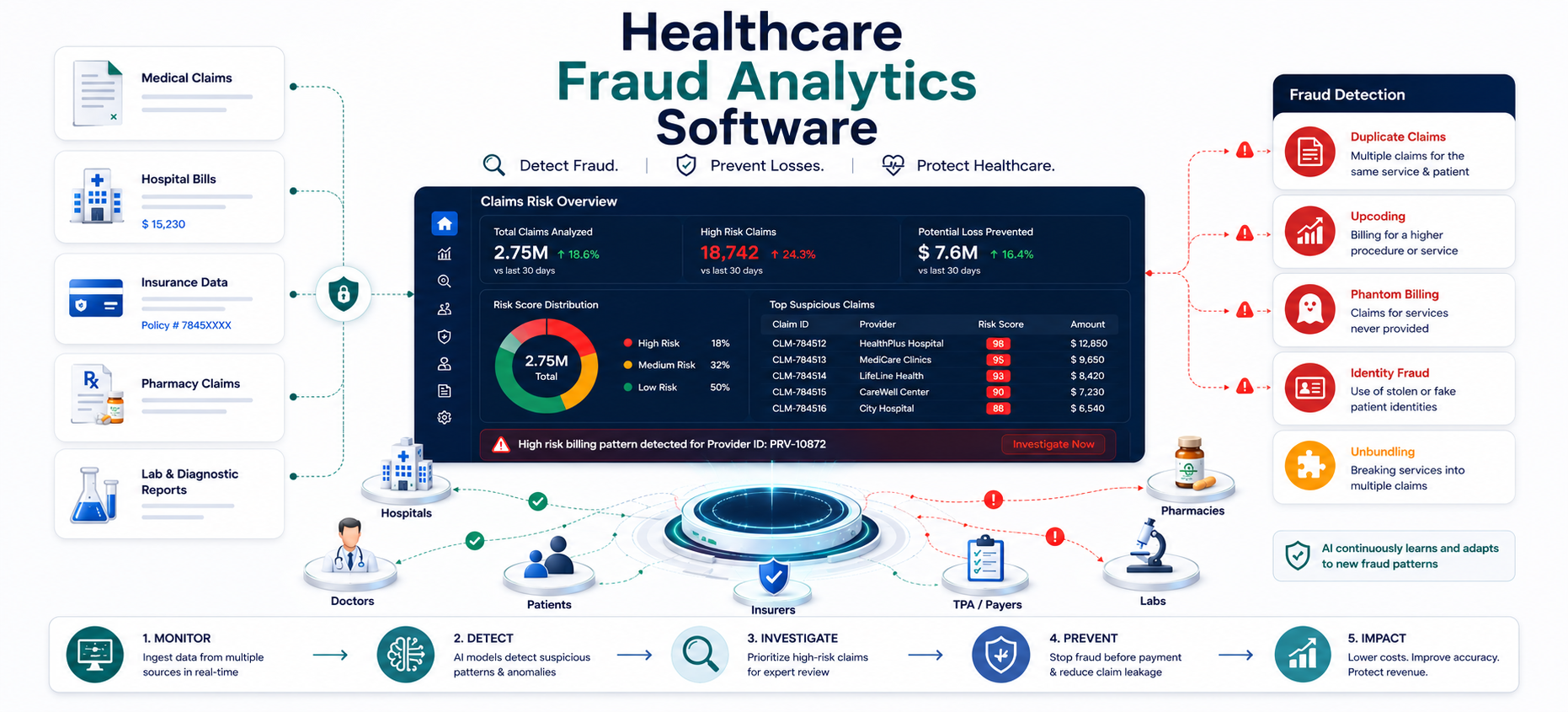
Fraud in health claims takes a few well-known shapes. Most fraud analytics platforms are built to watch for these patterns first:
- Duplicate claims — the same treatment billed across two policies, or resubmitted after it was already paid
- Upcoding — billing for a more complex or expensive procedure than what was actually performed
- Phantom billing — charges for admissions, tests, or surgeries that never happened
- Identity fraud — a claim filed under someone else's member ID, or with fabricated medical records
- Provider anomalies — a hospital or clinic with unusual admission rates, length of stay, or procedure mix compared to peers
- Length-of-stay inflation — genuine hospitalisation, but the bill stretches the days or room category to raise the payout
Under IRDAI's own classification, fraud falls into three broad buckets: policyholder or claims fraud, intermediary fraud, and internal fraud. Most of the patient-facing patterns above sit in the first bucket, and it is the one insurers see the most volume of.
IRDAI's 2026 Fraud Monitoring Framework: What Changed?
On October 9, 2025, IRDAI issued a new Insurance Fraud Monitoring Framework, replacing a circular that had been in place since 2013. It became effective on April 1, 2026, and it is a much bigger deal than the name suggests.
A few things are genuinely new compared to the old rules:
- It covers more than insurers. The 2013 circular applied only to insurers and reinsurers. The 2026 framework also covers corporate brokers, web aggregators, bancassurance partners, hospitals, and individual agents.
- Zero-tolerance is now a written requirement. Every insurer and distribution partner must adopt an explicit anti-fraud stance, not just a general compliance policy.
- Fraud Monitoring Committees are mandatory. These must be headed by a Key Management Personnel and staffed with senior people from underwriting, claims, legal, and technology — with quarterly reporting to the board.
- Five fraud categories, tracked separately. Internal fraud, claims fraud, distribution-related fraud, cyber fraud, and digital fraud each need their own detection and reporting approach.
- Red Flag Indicators must evolve. Insurers have to build and continuously refine a living list of fraud signals — unusual claim frequency, claims filed right after policy issuance, or documentation that does not match the policy terms — instead of relying on a fixed rulebook.
- Shared intelligence through the Insurance Information Bureau. Insurers now contribute fraud data to a common "caution repository" of flagged entities, so a provider blacklisted by one insurer is visible to others.
The message underneath all of this is simple: static, manual, once-a-year fraud checks no longer meet the bar. Regulators expect fraud detection to run continuously, at the point of claim submission, with a documented and auditable process behind every flagged case.
Health Insurance Fraud in India: Statistics and Industry Impact
India's health insurance market is growing fast — gross written premium is projected to cross US$246 billion across all insurance lines in 2026. Fraud is scaling right alongside it. Industry estimates put fraud, waste, and abuse losses at somewhere between 7% and 15% of gross premium in health insurance specifically, and separate industry research suggests roughly 15% of health claims carry some element of fraud.
Digitisation is a double-edged factor here. It has made claims faster to file and process, but it has also opened up new fraud vectors — fake portals, phishing, and coordinated fraud rings that simply did not exist when the 2013 rules were written.
Benefits of Fraud Analytics Software
Fraud analytics software and claims fraud analytics help insurers, TPAs, and hospitals identify suspicious claims, reduce financial losses, improve claims management, and meet regulatory requirements while maintaining a better experience for genuine policyholders.
Faster Fraud Detection
Automated fraud checks identify suspicious claims within seconds instead of relying only on manual reviews. This helps investigation teams focus on high-risk cases without delaying legitimate claims.
Reduced Financial Losses
By detecting duplicate claims, upcoding, identity misuse, and billing anomalies before payments are approved, fraud analytics software helps prevent unnecessary payouts and protects revenue.
Better Regulatory Compliance
Modern fraud analytics platforms support IRDAI's fraud monitoring framework by maintaining audit trails, documenting investigation workflows, and generating reports required for internal committees and regulatory reviews.
Improved Claims Processing Efficiency
Low-risk claims can move through the approval process more quickly while only suspicious claims are routed for additional investigation. This reduces processing time and improves customer satisfaction.
Smarter Decision-Making
As more claims are processed, fraud analytics software continuously builds insights into provider behaviour, billing trends, and fraud patterns. These insights help organizations refine fraud detection strategies and improve future decision-making.
How Fraud Analytics Software Works in Health Insurance
Modern health insurance fraud detection software combines rule-based checks with behavioural analysis, network intelligence, and machine learning to identify suspicious claims before payments are processed.
- Threshold rules — Predefined rules flag unusual claim amounts, extended hospital stays, frequent procedures, or other activities that exceed normal thresholds, helping identify claims that need further review.
- Cross-claim matching — The system compares claims to detect duplicate service dates, repeated provider IDs, shared contact details, and other similarities that may indicate duplicate billing or organised fraud.
- Diagnosis–procedure coherence checks — The software checks whether diagnosis (ICD) codes and billed procedures are clinically consistent. Claims with mismatched information are flagged for investigation.
- Network and relationship mapping — By analysing relationships between hospitals, providers, clinics, and patients, the system can identify hidden connections and potential fraud networks.
- Machine learning on historical fraud cases — Machine learning analyses historical claims and confirmed fraud cases to assign risk scores, helping investigators prioritise high-risk claims and improve detection over time.
None of these techniques work effectively in isolation. When integrated with claims systems, VMER records, hospital bills, and provider data, fraud analytics software gains the context needed to detect complex fraud before payments are made.
How NHCX Supports Health Insurance Fraud Detection
Running alongside the IRDAI framework is the National Health Claims Exchange (NHCX) — a digital platform built under the Ayushman Bharat Digital Mission to standardise how claims data moves between hospitals, TPAs, and insurers. NHCX matters for fraud detection for a specific reason: standardised, structured claims data is far easier to run automated checks against than the mixed PDF-and-paper submissions many insurers still process today.
Uniform data formats and centralised validation, as NHCX rolls out further, are expected to reduce the manual document-chasing that fraud tends to hide inside. It will not replace an insurer's own fraud analytics — but it does make automated detection more reliable once claims arrive in a consistent format.
Catching Fraud Before Payout, Not After
Post-payout recovery in Indian health insurance is slow, legal-heavy, and often only partially successful. The real economic win is holding suspicious claims for analyst review while auto-approving clean, low-risk claims fast — so honest hospitals and policyholders are not caught up in the friction.
Every rupee paid on a fraudulent claim is a rupee not available for honest policyholders. Pre-payout detection costs a fraction of post-payout recovery — which often yields nothing at all.
This is where fraud scoring needs to sit inside the claims workflow itself, not bolted on afterward. Plugging fraud analytics into RCM automation at the point of submission means scoring happens before funds move, not after.
Why Hospitals Also Need Fraud Analytics Software
Hospitals are frequently victims of fraud too, not just facilitators of it. Internal billing errors — duplicate charge lines, incorrect package mappings, missing documentation — trigger insurer audits, delayed payments, and even empanelment risk for hospitals that did nothing wrong on purpose. Running fraud and anomaly checks on the provider side, before bills go out, protects a hospital's own revenue integrity and its standing with insurers.
This works best when clinical documentation actually backs up what gets billed. A structured EMR from hospital information management software makes sure the treatment record supports the claim under scrutiny, instead of leaving gaps that look like fraud even when they are not.
Key Features of Fraud Analytics Software
Most teams evaluating fraud analytics start by asking for "a dashboard." That undersells what a proper build needs to do. A useful fraud analytics engagement usually covers eight connected pieces, not one:
- Billing pattern analysis — modelled on your own claims history, so "unusual" is defined against your real billing cycles, provider specialty patterns, and claim sequences, not a generic industry template
- Anomaly-detection workflows — automated flags for statistical outliers in service frequency, billing amounts, diagnosis combinations, and procedure clusters, routed to your review team for confirmation
- Configurable alerts — thresholds your own team controls, delivered by email, SMS, or dashboard, timed around how your claims review process actually works
- Claims deep-dive analysis — checks tuned to the specific issues you care about, correlating duplicate claims, unbundling, and upcoding signals across time, providers, and patient records
- Provider risk scoring — risk profiles built from historical provider behaviour and claim patterns, so your team can prioritise monitoring and targeted audits instead of reviewing everyone equally
- Relationship mapping — network views connecting providers, clinics, patient groups, and billing entities, useful when investigators need to see connected parties in one place
- Review and case workflows — document review, timelines, and evidence collection built as a structured workflow with audit trails, not a spreadsheet passed between analysts
- Reporting outputs — formats built for your internal committees, payers, or regulators, gathered during scoping so reports match what your Fraud Monitoring Committee actually needs to see
This is exactly the scope CSoft combines claims analytics software with fraud detection workflows to help organisations identify anomalies, monitor billing patterns, and investigate suspicious claims more efficiently.
How Fraud Analytics Software Helps Meet IRDAI Compliance
The new framework is not just about catching more fraud — it is about proving you can. Fraud Monitoring Committees need quarterly reporting. The Insurance Information Bureau needs standardised data contributions. And any claim that gets escalated needs a documented trail showing why it was flagged, who reviewed it, and what evidence supported the decision.
This is where a lot of off-the-shelf fraud tools fall short — they generate alerts but not audit-ready case files. A properly scoped build closes that gap in a few specific ways:
- Every flagged claim carries a documented reason code and scoring logic, not just a "high risk" label
- Case management screens capture reviewer notes, timelines, and evidence in one place, ready to hand to a compliance officer or regulator on request
- Reporting formats are agreed during scoping so committee-ready reports come out of the system, instead of being rebuilt manually before every board meeting
Because CSoft builds these workflows around your existing ABDM interoperability layer, audit trails stay connected to the original claims and clinical records they came from, which matters when a regulator or insurer questions a specific case months later.
Custom vs Off-the-Shelf Fraud Analytics Software
A generic fraud detection product ships with rules tuned to someone else's claims data, someone else's provider mix, and someone else's fraud history. Applied directly to your claims, it tends to do one of two things: flood your review team with false positives, or miss the fraud patterns specific to your market.
CSoft's approach to fraud analytics is deliberately different, and it is worth explaining why it matters for outcomes, not just as a sales point:
- Built per client, not off the shelf. Every dashboard and detection rule is designed around your claims data, your review process, and the patterns your team already flags manually.
- Roadmap-led enhancement. Builds typically start with dashboards and rule-based checks, then add model-based detection as your data and confidence grow — the roadmap is agreed together, not imposed upfront.
- Tuned to limit false positives. Detection rules are calibrated against your legitimate billing patterns and refined with your reviewers' feedback, so investigators are not flooded with noise and honest providers are not wrongly flagged.
- Built on your VMER/RCM foundation. Because the analytics extension connects natively to CSoft's ready VMER and RCM products, claims data flows in without a separate platform project or a second integration effort.
The practical effect: expected savings and detection targets get estimated honestly during scoping, based on your actual claims volume, instead of a vendor's generic benchmark from a different market.
Fraud Analytics Implementation Checklist for Insurers, TPAs, and Hospitals
With the April 2026 deadline already in effect, most of the framework's requirements are no longer future planning items — they are live compliance obligations. A practical starting checklist:
- Confirm a Fraud Monitoring Committee is formally constituted and reporting to the board quarterly
- Document a board-approved Anti-Fraud Policy covering all five fraud categories, not just claims fraud
- Map your current Red Flag Indicators and set a cadence for refreshing them
- Check whether your claims data is structured enough to feed automated cross-claim matching, or whether it is still trapped in scanned documents
- Decide where fraud scoring sits in your claims pipeline — ideally before pre-authorisation, not after
How CSoft Fraud Analytics Helps Prevent Insurance Fraud
CSoft Fraud Analytics scores claims at submission using cross-referenced VMER records, hospital bills, and provider patterns — routing high-risk cases to investigation before payout, and built on CSoft's ready VMER/RCM foundation so it connects into your existing claims workflow instead of requiring a separate platform. Engagements are scoped around your claims data first, so the dashboards, alert thresholds, and reporting formats you get back are built for how your team actually reviews cases — not a generic template.
Book a demo or talk to us on WhatsApp to discuss a fraud analytics scope for your organisation.